Arthrocentesis is a relatively benign procedure, and if properly performed, complications are rare. Potential complications include iatrogenic infection, localized trauma, pain, and reaccumulation of the effusion
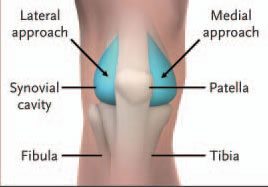
Failure to aspirate synovial fluid results in a “dry tap.” Misdiagnosis of knee effusion, obesity, obstruction of the needle lumen by particulate matter or a plica, or hypertrophy of the synovium (owing to chronic inflammation) may all result in a dry tap. If the medial approach was used initially, a lateral approach should be attempted, since this may overcome difficulties presented by a medial plica or thick medial fat pad.
Collected fluid should immediately be placed into appropriate containers and analyzed expediently. Check with the laboratory regarding specific submission procedures (e.g., the correct tubes and the volume of fluid required for each test). If only minute volumes of synovial fluid are obtained, discussions with laboratory personnel are indicated to prioritize testing. As little as one drop of fluid may be sufficient for crystal analysis, and 1 ml may suffice for a cell count and a differential count.
Gram’s staining and culture of synovial fluid provide the most definitive evidence of septic arthritis. The sensitivity of these techniques is much higher for nongonococcal infections (50 to 75 percent for Gram’s staining and 75 to 95 percent for culture) than for disseminated gonococcal disease (less than 10 percent and 10 to 50 percent, respectively.) If gonococcus is suspected, cultures of the blood and of urethral, rectal, or oropharyngeal swabs should be considered. To minimize the risk of contamination, the synovial fluid is often submitted for testing in the syringe used for the arthrocentesis.
The cell count and differential count are used to differentiate between non inflammatory effusions (e.g., osteoarthritis and trauma) and inflammatory conditions (e.g., septic and crystal-induced arthritis). A cutoff of 2000 white cells per milliliter and 75 percent polymorphonuclear cells is generally used. It should be emphasized that the cell count and differential count cannot reliably differentiate among various inflammatory entities. For example, up to 33 percent of patients with septic arthritis may have white-cell counts below 50,000 per milliliter, and patients with acute gouty arthritis may have counts exceeding 100,000 per milliliter. Synovial fluid is usually submitted for cell and differential counts in specimen tubes treated with EDTA.
Evaluation of synovial fluid under a polarizing-light microscope may reveal the presence of monosodium urate crystals (seen in gout) or calcium pyrophosphate dihydrate crystals (seen in pseudogout). The sensitivity of crystal analysis is relatively high (80 to 95 percent for gout and 65 to 80 percent for pseudogout). It should be noted that the presence of crystals does not exclude the possibility of septic arthritis, since the two conditions may coexist. Synovial fluid is usually submitted for crystal analysis in a lithium heparin–treated specimen tube.
Although often ordered, biochemical assays such as for glucose, protein, and lactate dehydrogenase have little discriminatory value and should not be included in routine synovial-fluid analysis. Other tests, such as specific stains and cultures for atypical infectious agents and cytologic evaluation for suspected malignant effusions, may be indicated in certain situations.
n engl j med 354;19 www.nejm.org may 11, 2006